What Causes BPD in Women: Risk Factors & Triggers Explored
If you’ve been searching what causes BPD in women, you’re probably looking for clarity—not blame—around intense emotions and relationship patterns. This guide explains what causes BPD in women in terms of common risk factors and life experiences that may increase vulnerability, along with the difference between root causes and everyday triggers. It’s for education and self-understanding, not a diagnosis or treatment plan. If you also want a gender-related perspective on how symptoms can be recognized differently, you can read our guide on BPD symptoms in men.

What is Borderline Personality Disorder (BPD)?
Before exploring causes of BPD in females, it helps to define what BPD is. Borderline Personality Disorder is a mental health condition marked by persistent patterns of emotional instability, shifting self-image, and relationship difficulties. It’s not simply being “emotional”—it’s often about how strongly emotions surge and how hard they can be to regulate in the moment.
A Quick Look at the Core Symptoms
People who meet criteria for BPD may experience emotions that shift quickly and feel overwhelming. This is often what BPD can look like in females (and in people of any gender), especially when stress or relationship tension is present. Common patterns clinicians look for include:
- An intense fear of abandonment (real or perceived).
- Unstable, intense relationships that swing between closeness and conflict.
- An unclear or shifting sense of self.
- Impulsive behaviors that can create regret or risk.
- Chronic feelings of emptiness.
- Intense anger or difficulty calming down once upset.
Why BPD Is More Than Mood Swings
Everyone’s mood changes sometimes. With BPD, emotional shifts tend to be more intense, more frequent, and more tightly connected to interpersonal stress—like feeling rejected, criticized, or left out. Over time, that emotional reactivity can affect work, friendships, and identity.
If you suspect these patterns may apply to you, a qualified clinician can help clarify what’s going on and discuss evidence-based supports. Many people benefit from skills-focused approaches (such as DBT-style emotion regulation and relationship skills), but the right support depends on your situation.
Core causes of BPD in Women: Biological Risk Factors
There isn’t a single answer to what causes BPD in women. Most researchers describe BPD as developing from a combination of vulnerabilities and experiences. In many cases, biology may contribute to a person’s baseline sensitivity—how intensely they feel emotions and how quickly their stress system reacts.
Genetic and Hereditary Factors
Is BPD hereditary? Research suggests genetics can play a role. Having a close family member with BPD or related traits may increase risk, but it does not mean someone will develop BPD. Genes are better understood as a predisposition—one part of a larger picture that also includes environment, learning, and relationships.
Brain Structure and Function Differences
Brain research has explored differences in areas involved in emotion and impulse control. Findings vary across studies, but some patterns have been observed in regions related to threat detection, regulation, and memory. In simple terms, the brain systems that signal danger may react strongly, while the systems that help “slow things down” may not engage as easily under stress.
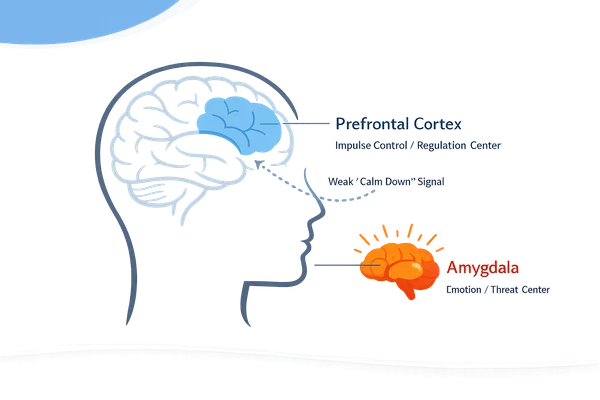
These kinds of differences may help explain why emotions can feel so intense and urgent for some people—especially in moments of perceived rejection or instability.
Core causes of BPD in Women: Environmental and Childhood Risk Factors
Biology may set the sensitivity level, but environment often shapes how someone learns to handle emotions, relationships, and self-worth. This is where many childhood causes of borderline personality disorder are discussed—not as “one event causes BPD,” but as repeated experiences that may affect emotional development over time.
The Impact of an Invalidating Childhood Environment
An invalidating environment is one in which a child’s feelings are repeatedly dismissed, ignored, punished, or treated as “too much.” Over time, a child may learn that emotions are unsafe, unacceptable, or unreliable.
In practice, this can interfere with building steady self-trust and healthy emotion regulation. It can also make relationship security feel fragile later in life, because emotional needs were not consistently met or understood.
How Childhood Trauma Contributes as a Risk Factor
Childhood trauma is frequently reported among people diagnosed with BPD, though experiences vary widely. Trauma can include abuse, neglect, chronic conflict at home, or a major early loss. Growing up with caregivers struggling with mental health concerns or substance use may also create instability.
These experiences may affect attachment (how safe relationships feel), threat sensitivity, and coping habits—factors that can contribute to BPD vulnerability. That said, not everyone with trauma develops BPD, and not everyone with BPD reports a clear trauma history.
Why is BPD Diagnosed More Often in Women?
Many people wonder: why is BPD more common in females in diagnosis statistics? One explanation is that women may be diagnosed more often, not necessarily because they “have it more,” but because symptoms can be recognized, interpreted, and expressed differently across genders.
The Role of Diagnostic Bias in Clinical Settings
Historically, BPD was often viewed through a gendered lens. That can influence which labels clinicians consider first. For example, when someone shows anger, impulsivity, or relationship conflict, different diagnoses may be explored depending on presentation, context, and bias.
This matters because diagnostic pathways can shape access to appropriate care. If BPD is missed, people may not get the skills-focused supports that target emotion regulation and relationship patterns.
How Symptoms May Present Differently in Women
Social expectations can influence coping styles. Some women are more likely to internalize distress, which can show up as self-criticism, self-harm urges, emptiness, or identity confusion—often discussed as symptoms of BPD in females. Some men may externalize distress through anger, risk-taking, or substance use, which can lead clinicians to consider other diagnoses first.
Because of this, it can help to focus on underlying patterns (emotion regulation, fear of abandonment, identity instability), not only on how distress looks on the surface.
What's the Difference Between Root Causes and Daily Triggers?
Understanding “cause” versus “trigger” can make the whole topic feel more manageable. Causes are long-term factors that shape vulnerability. Triggers are the immediate sparks that set off a strong reaction.
People often ask: What triggers BPD mood swings? In many cases, triggers are interpersonal and connect to core fears—like abandonment, rejection, or being misunderstood.
Causes: The Foundation of Vulnerability
Root causes are the slow-building influences we discussed—biological sensitivity plus formative experiences (especially in childhood). You usually can’t change your genetics or rewrite your past, but understanding these influences can reduce shame and self-blame.
Triggers: The Spark for a Reaction
Triggers happen in the present: a look, a tone of voice, a delayed reply, a sudden change of plans. They don’t “create” BPD, but they can activate intense feelings that are already easier to ignite due to the underlying vulnerability.
Common Examples of BPD Triggers
Triggers are personal, but many fall into recognizable categories:
- Perceived rejection: A friend not texting back quickly.
- Criticism or feedback: Even when meant to be constructive.
- Relationship transitions: A partner traveling or needing space.
- Feeling dismissed: Someone minimizing your emotions.
- High stress: Big changes at work, school, or home.
How Can You Start to Make Sense of Your Own Patterns?
After learning about possible causes and triggers, it’s normal to reflect on your own experiences. The goal here is not self-diagnosis—it’s building self-awareness so you can describe patterns clearly and choose next steps that feel supportive.
A Quick Checklist for Self-Reflection
Use these questions as a gentle guide. You don’t need to answer “yes” to everything for your experiences to be real or worth support.
- Emotional intensity: Do emotions feel sudden or overwhelming?
- Relationship patterns: Do relationships feel intensely close, then suddenly shaky?
- Fear of abandonment: Does distance from someone feel catastrophic?
- Sense of self: Do you feel unsure who you are across different situations?
- Impulsivity: Do you act quickly in ways you later regret?
A Structured Screener You Can Use as a Conversation Starter
If you want a more structured way to reflect, you can try our free BPD screening quiz. It’s designed to help you organize thoughts about common BPD-related patterns in a private, low-pressure way.
Disclaimer: This is an educational screener, not a diagnostic test. Only a qualified mental health professional can diagnose BPD, and results should be used as a starting point for reflection and conversation—not a conclusion.
When to Consider Professional Support
Consider reaching out for professional help if you notice any of the following:
- Your emotions feel unmanageable or lead to frequent conflict.
- Relationship instability is causing major distress.
- You have urges to self-harm, act dangerously, or you feel unsafe.
- Symptoms interfere with work, school, sleep, or daily functioning.
- You feel stuck in repeated cycles and want tools to change them.
Your Path Forward: From Understanding to Seeking Support
Exploring what causes BPD in women can be a meaningful step toward compassion and clarity. In many cases, BPD vulnerability reflects a mix of emotional sensitivity and early experiences that shaped coping and attachment—not a personal failure. Knowing this can shift the question from “What’s wrong with me?” to “What patterns have I learned, and what do I need now?”
If you’d like a structured way to organize your thoughts before talking with a clinician, you can also explore our BPD test online. And if you’re already working with a therapist, the most helpful next step may be bringing these patterns and triggers into the room so you can build skills and support around them.
Frequently Asked Questions about BPD Causes
Can you have BPD traits without having the full disorder?
Yes. Many people have a few BPD-related traits without meeting diagnostic criteria. A diagnosis usually requires patterns that are persistent, widespread across contexts, and cause significant impairment or distress. If you’re unsure, a clinician can help you sort it out.
How are the causes of BPD different from those of Bipolar Disorder?
Bipolar disorder is defined by episodes of depression and mania/hypomania that can last days to weeks. BPD mood shifts are often faster and closely tied to interpersonal stress and fear of rejection. Only a professional assessment can determine which pattern fits best.
Can you develop BPD without a history of trauma?
Yes. Trauma is a common risk factor, but it isn’t required. Some people develop BPD patterns through chronic invalidation, inconsistent caregiving, or long-term stress, especially when combined with high emotional sensitivity. A clinician can help explore your history safely.
Does understanding the causes of BPD help in managing it?
Often, yes. Understanding possible causes can reduce shame and help you notice triggers earlier. That awareness can support better coping choices, communication, and seeking appropriate help. It won’t replace treatment, but it can make your next steps clearer.